
QVI Home > Case of the Month
|
QVI Case of the Month! For past cases, click here
PATIENT HISTORY: An 82-year-old female presents with a history of lung malignancy currently undergoing chemotherapy. Two days ago she developed left calf pain in the leg began to swell noticeably yesterday and she was referred to us with suspicion of venous thrombosis. She denied prior DVT or SVT and gave up tobacco April 2009.
PHYSICAL EXAM: The left leg is notably swollen compared to the right leg and measurements are as follows: Right calf 12 ½”, right ankle 8 ", compared to the left calf at 14 ", and left ankle 8 ¾”. There were no significant varicosities and only a few spider and reticular vein clusters present. Popliteal and ankle pulses are palpable bilaterally.
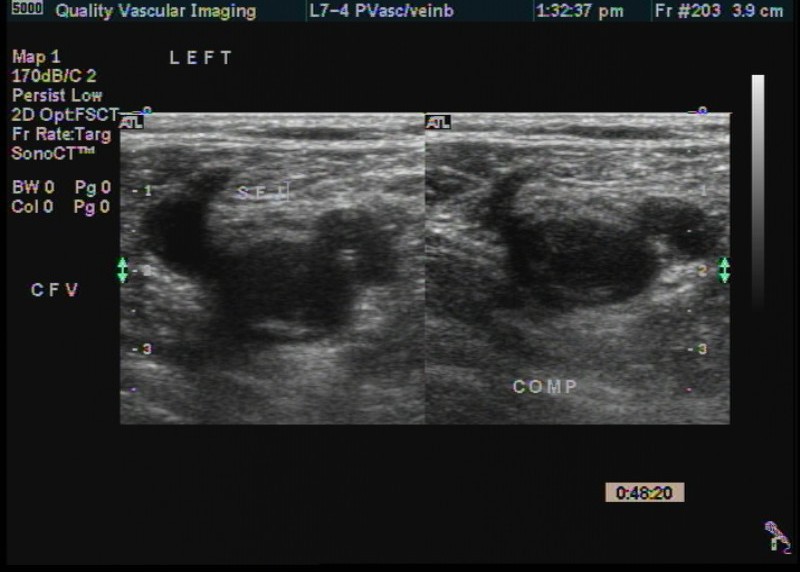
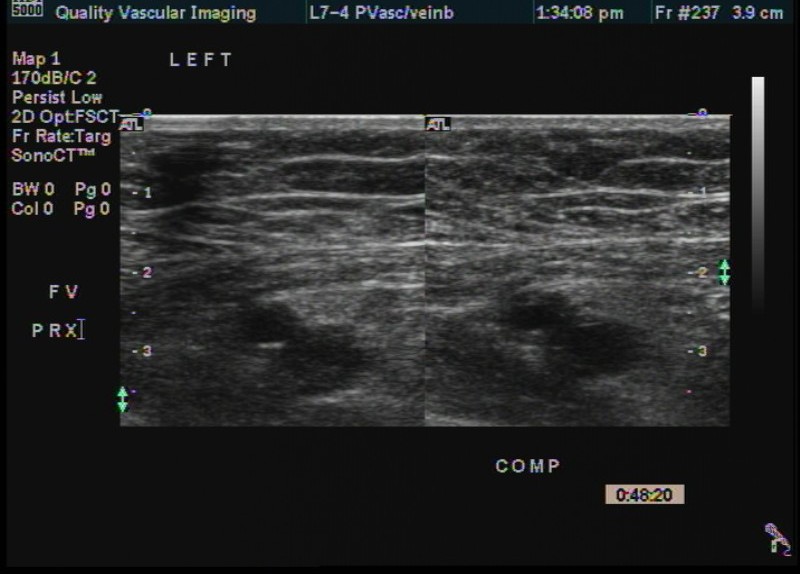
Left Leg Images-
Obvious left femoral popliteal and tibial thrombosis but note the abnormal, largely continuous flow pattern in the common femoral and saphenofemoral junction.
Right Leg Images -
Note - some respiratory phasicity present
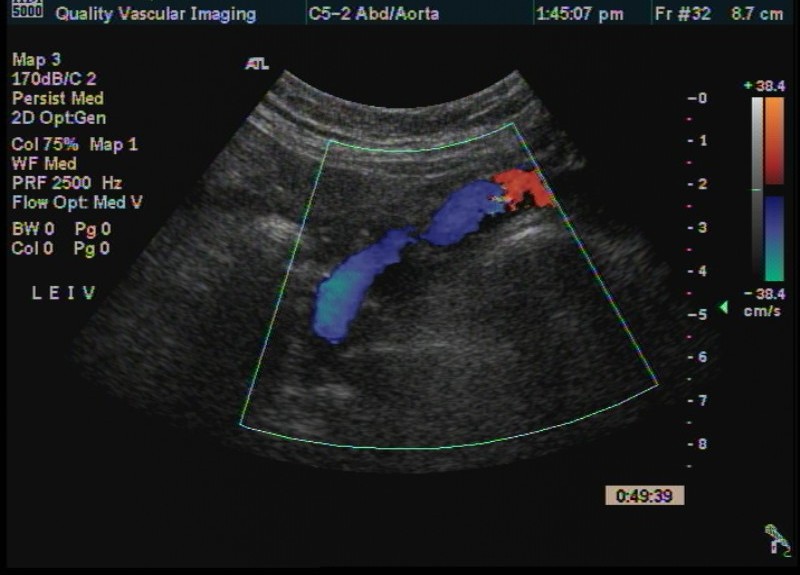
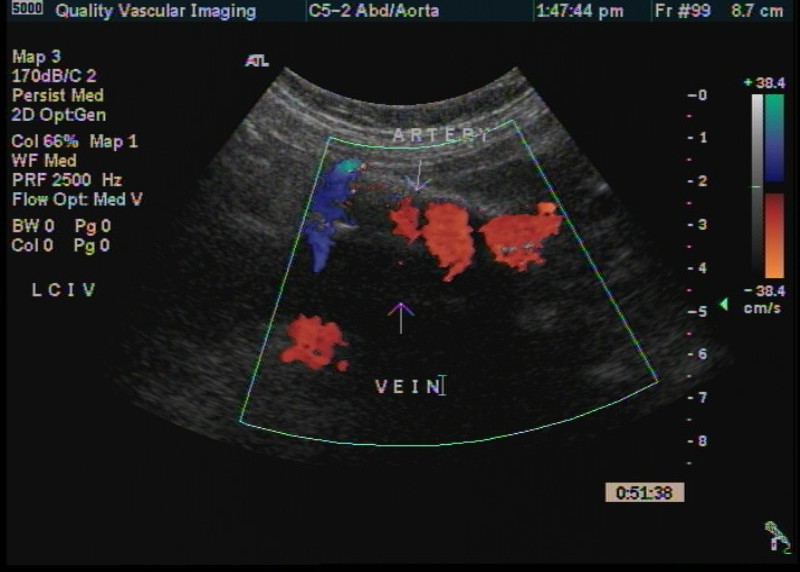
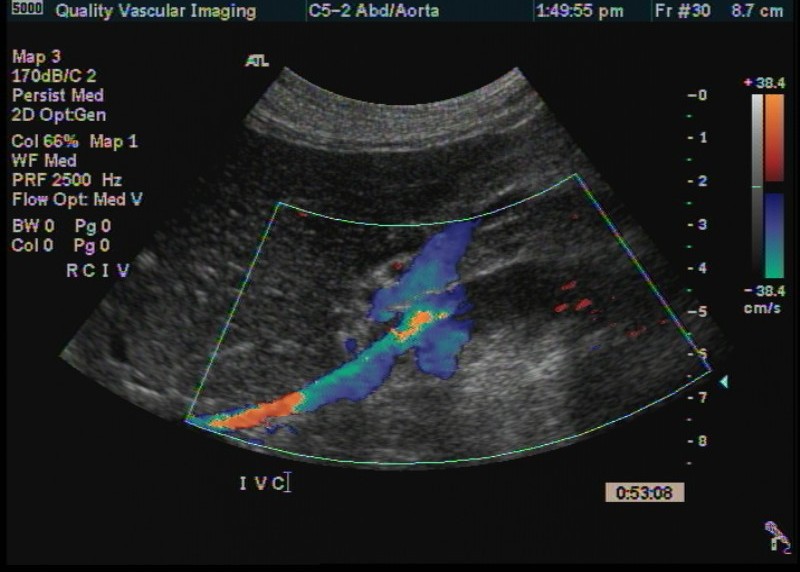
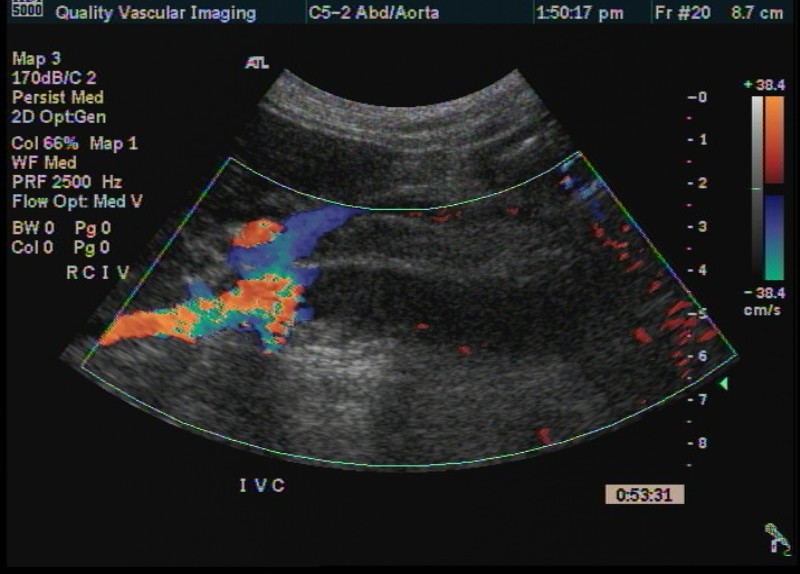
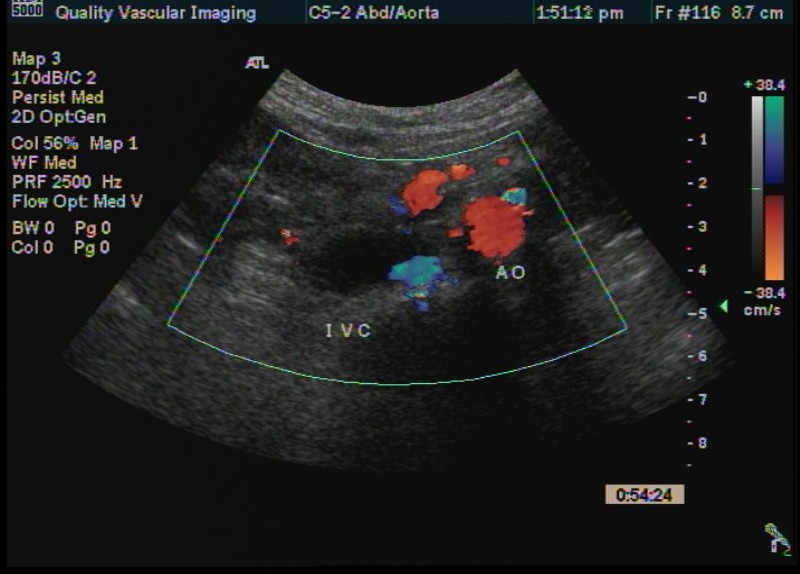
Pelvic and Abdominal Veins
Note the continuous flow in the left external iliac vein in contrast to some respiratory phasicity of the right external iliac vein albeit somewhat dampened.
Some suspicion for partial obstruction in the left external iliac vein. Not the highest quality image of the left common iliac vein but appears to be completely obstructed. There was also some suspicion of partial obstruction of the right common iliac vein.
The distal inferior vena cava is slightly distended and nearly completely obstructed. The transverse image demonstrates a small persistant lumen with flow from the right common iliac vein. The left renal vein is identified and the IVC is widely patent above this confluence but largley obstructed distal to this.
Discussion:It is no mystery that patients with malignancy and especially those undergoing chmotherapy are at exceptionally high risk for venous thrombosis. This case is somewhat unusual in that the patient had only been symptomatic for 48 hours and presents with such extensive thrombosis. The vascular technologist needs to be aware of normal and abnormal flow patterns on the outflow veins of the leg and comparison between the right and left legs is critical in the evaluation of patients suspected of having acute venous thrombosis. Given persistant respiratory phasicity, the extent of the thrombus into the IVC with a nearly complete obstruction was somewhat unexpected.
QVI Case of the Month! For past cases, click here
|
QVI Home Virtual Vein Center Why QVI really is the Best in Vascular Ultrasound! Case of the Month Patients Referring Physicians Health Professionals Site Map |














Compression Socks?
We carry the BEST!

Compression socks are not only a main stay in the treatment of venous and lymphatic disease but are now used by elite athletes everywhere. Please visit our webstore for more information about compression therapy by clicking the image above! .